
Health care-acquired infections (HAIs) are infections that are acquired in hospitals or other health care settings. These are also called nosocomial infection and can occur in hospitals, nursing homes, rehabilitation facilities, and other ambulatory care facilities. Health care designers are sometimes misguided and believe that HAIs only occur in hospital settings. For this reason, HAIs are sometimes referred to as health care-associated infections to account for areas such as ambulatory care facilities.
The Center for Medicare and Medicaid Services stated that HAIs are among the leading causes of preventable deaths in health care environments and are associated with a substantial increase in health care costs each year. Common HAIs patients get in hospitals include central-line associated bloodstream infections (CLABSI), clostridium difficile infections, pneumonia, methicillin-resistant Staphylococcus aureus (MRSA) infections, surgical site infections, and urinary tract infections. Catheter-associated urinary tract infections (CAUTI) are some of the most common HAIs. The Centers for Disease Control and Prevention (CDC) states that HAIs kill more people in this country than AIDS, breast cancer, and auto accidents combined.
Some of the most dangerous HAI pathogens are those that have the potential to spread by the airborne route (Kowalski 2006). Many of these pathogens are now called “superbugs,” because they are virtually resistant to standard drug treatment. One of the most common is methicillin-resistant Staphylococcus aureus (MRSA). Poor indoor environments in ambulatory care facilities tend to self-perpetuate these agents, which add to the concern of infection control specialists everywhere. Addressing the infection control in ambulatory facilities requires integrating HVAC and good air-pressure control with dedicated infection-control systems as well as minimizing unplanned airflows through building envelopes and interior spaces.
The first step in addressing HAIs that are airborne is to ensure proper air filtration of the airflow in the HVAC systems. Good air filtration of outside air and mixed air that is being introduced to the ambulatory care facility is the primary means of reducing the concentrations of airborne bacteria that cause HAIs. Studies have shown that 99.9 percent of airborne bacteria in hospitals are removed by high-efficiency MERV-14 filters in the AHUs serving the spaces.
ASHRAE Standard 170-2017, Ventilation of Health Care Facilities, as a minimum, requires two levels of filtration for patient care areas: the first filter upstream (MERV 8) of fans and coils and the second filter downstream (MERV 14) of the cooling coils and supply fan. However, outpatient surgical platforms that comply with these minimum air-filtration requirements still record several cases of HAIs, which resulted in huge hospital payouts. It is important to note that ASHRAE’s ventilation standards only stipulate minimum requirements and, therefore, it is up to the health care engineer to specify the appropriate air filtration for areas susceptible to airborne infection.
ASHRAE Standard 170-2017 requires high-efficiency particulate air (HEPA) filters for protective environment and isolation rooms designed for patients with high susceptibility to infections and patients that can spread communicable disease. The standard does not discuss the use of any enhanced filtration in the air system for outpatient operating rooms. As health care engineers, we need to acknowledge the risk of doing the minimum and the impact it can have on patients and health care facilities. There are many types of air filtration technologies that are available that will minimize the occurrence of HAIs. As a minimum, all surgical space in an ambulatory care facility should contain HEPA filtration — either at the AHUs or local to the operating rooms. Other enhanced air-filtration technology can be specified for the air system to enhance the filter efficiency and reduce the occurrence of HAIs.
Filter Selection
During HVAC design of ambulatory care facilities, there are several factors that influence filter selection, including pressure drop, energy usage, projected filter life, ease of installation, and speed of the airflow in the HVAC unit. Filter selection is a balancing act for health care engineers, because it deals with a combination of first cost and long-term operation cost associated with the filter that is selected. When the filter section factors are considered, the more expensive filter in initial cost will most likely have the least operation cost.
 FIGURE 1. Table 6.4 from ASHRAE 170-2017, Minimum Filter Efficiencies.
FIGURE 1. Table 6.4 from ASHRAE 170-2017, Minimum Filter Efficiencies.
Filter test results vary significantly, and it is always a good idea to insist that all filters being considered are supported by testing of an independent third-party laboratory. The best way to assess which filter to use is to work with someone with extensive knowledge of filtration, such as an individual with a Certified Air Filter Specialist (CAFS) designation from the National Air Filtration Association (NAFA). Conversely, the best way to select a filter is to leave it to the filter manufacturers who usually have many CAFS specialists on their team. However, the engineer should be very careful to ensure that he or she fully understands the types of filters that are selected for the AHU, the pressure drop over the life of the filters, how the filters will affect the energy efficiency of the unit, and their maintenance requirements.
Pre-Filters
Most spaces in health care facilities require pre-filters. Per ASHRAE 170-2017, there are only a few areas of a health care facility that do not call for pre-filtration of areas that require high-efficiency filters. For health care facility designs, whenever there are filters of MERV 13 or above, it is a good idea to use a pre-filter to capture the larger particles. This extends the life of the high-efficiency filters and preserves the integrity of the second filter bank for capturing smaller particles. When you consider the high-efficiency MERV-13-and-above filters cost anywhere from 10-40 times the cost of a pleated filter (MERV-8 pre-filters), it’s easy to see the savings involved. Changing pleated filters on a quarterly basis is more economical than replacing a higher cost final filter six months prematurely because it had been used to remove large particles that could have been removed by pre-filters.
Location of Final Filters
The final filter location in an AHU has been debated throughout the industry for a long time. Some guidelines are still split on the final filter location. However, ASHRAE 170-2017 stipulates the final filter should be downstream of the coils. It does not stipulate the location of the pre-filter, but best engineering practice is to place it before the blower and coils. This arrangement ensures that the first filter bank captures the larger particles and is used to protect the equipment from dirt and other contaminants in the airstream. The second filter bank captures anything that makes it through the first filter or comes off the AHU itself. This is particularly important for older units whose coils may have mold on them. The second filter bank would capture the mold spores before they could enter the health care facility.
Proper Filter Installation
Ambulatory care facilities can have the best filter selection, but improper filter installation can lead to poor filter efficiencies and effectiveness. It’s important to properly install filter holding frames. They should be durable and sized to provide an airtight fit within the AHUs or ductwork. High-efficiency filters that are used in health care facilities have higher resistance, and are therefore more susceptible to the problems of air bypass. Any gaps between filter frames and between filters and the AHU doors and panels can create efficiency loss. For example, in a study conducted by Dr. Jeffrey Siegel at the University of Texas in Austin, it was found that just a 10-millimeter gap between filters could reduce filter efficiency from a MERV 15 to a MERV 8. This is even more critical for health care facilities because that means that HVAC units with these issues will be more susceptible to airborne infection.
Before the AHU is shipped to the health care facility for installation, it should be properly leak-tested to ensure the leakage is within the specified range, including the filter and filter frames. All joints between filter frame banks and the enclosing ductwork should be properly sealed to provide a positive seal against air leakage. Gaskets should be specified to be placed in the space between the last filter in the row and the filter bank door and between high-efficiency filters. Gasket material is made from neoprene or some other compressible, rubber-like material that will provide an airtight seal. It usually has an adhesive on one side protected by a peel-off backing. When designing an ambulatory care facility, it’s very important that the AHU specification include the installation requirement for the project.
Use Filter Pressure Measurement Device
A filter pressure measuring device should be installed across each high-efficiency filter bank (MERV 13 and MERV 14). These devices measure the pressure change in the AHU upstream of the filter to downstream of the air filter. Pressure gauges can give the facilities engineers important information about the filters in a system. Initial pressure drop significantly below what is expected from manufacturer’s specifications usually indicates the filters have not been installed properly and/or are not adequately sealed.
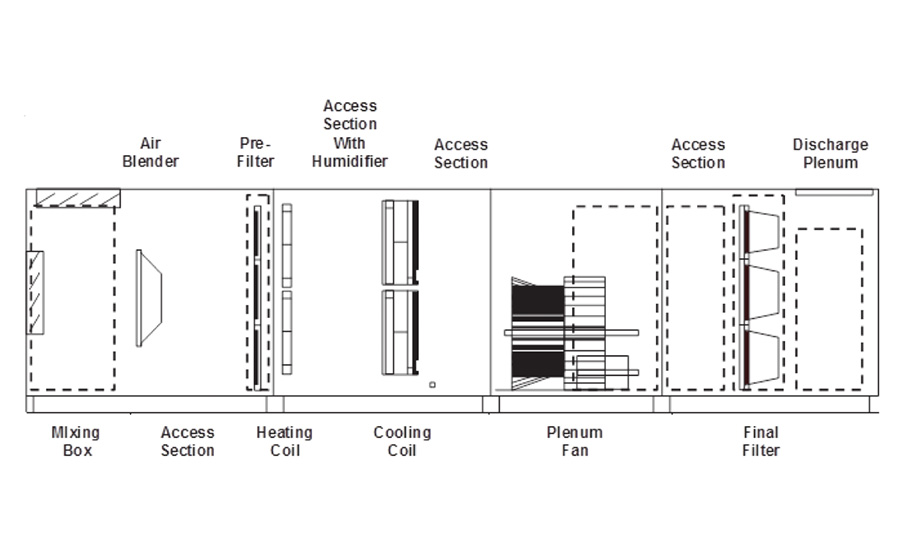 FIGURE 2. Typical air handling unit for outpatient surgery centers.
FIGURE 2. Typical air handling unit for outpatient surgery centers.
The filter measuring device is also a pressure drop indicator, and these are used to determine when a filter should be changed in the AHUs or other HVAC units in the health care facility. Air filter measuring devices are not installed on pre-filter banks because the filters are cheaper and are changed on a regular basis. However, for high-efficiency filters they are changed every six months and even sometimes only once per year. That said, some health care facilities are changing high-efficiency filters more often because of the presence of other contaminants, such as ozone, that can cause poor indoor air quality. The pressure change in the filter measuring device can be used as an important indicator for when the filter should be replaced. As the filter loads, with time, the concentration of contaminants increases. The best practice approach is to change the high-efficiency filters when the pressure drop doubles from its initial pressure drop.
Conclusion
The selection of the right filtration system plays an important role in minimizing the transfer of airborne diseases within the ambulatory care facility. The health care engineer is responsible for ensuring that the correct level of filtration is chosen not only to meet code requirements but also to minimize the risk of airborne infection through the HVAC systems. The design team and owner have the combined responsibility to determine whether enhanced filtration should be implemented for some specialty areas in the ambulatory care facility. Ambulatory care facilities are not different from hospitals when considering the level of filtration. All critical spaces in any health care setting need to have the proper filtration design in order to minimize airborne infection and, by extension, health care associated infection.




